
The COM-B framework and its use in explaining non-adherence
For patients with pancreatic exocrine insufficiency, there are a variety of reasons why they may not adhere to treatment. Some of these are modifiable.
There is therefore a need for a comprehensive framework that assesses and understands adherence.
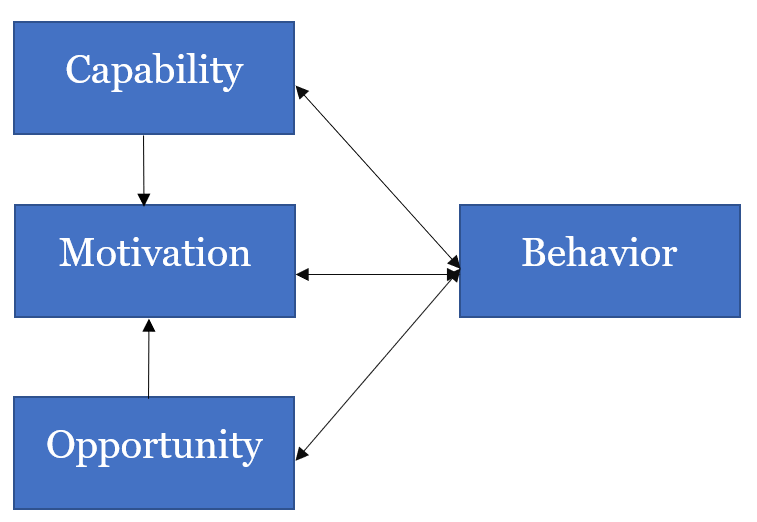
COM-B is a framework that encompasses Capability, Opportunity and Motivation, allowing a precise understanding of the relationship between the individual and adherence.
A comprehensive framework for the assessment of adherence is needed
Non-adherence is multi-faceted. Systematic reviews have suggested many reasons why patients may not adhere to their treatments.1 Some of these may be modifiable, such as patient understanding of their condition and the support available to them, and others may be fixed (such as the age and gender of the patient).1
A review of 51 such systematic reviews, assessing non-adherence to therapies for chronic diseases in 19 categories, identified over 750 individual factor items. The majority of these were linked to the implementation of treatment, with a small proportion related to persistence.1
A review of 51 such systematic reviews, assessing non-adherence to therapies for chronic diseases in 19 categories, identified over 750 individual factor items. The majority of these were linked to the implementation of treatment, with a small proportion related to persistence.1
| Term | Definition |
| Treatment implementation1 | How well a patient’s dosing corresponds to the prescribed dosing regimen |
| Persistence1 | The length of time between starting the medicine and taking the final dose before discontinuation |
A large proportion of patients receiving treatment with PERT for pancreatic exocrine insufficiency may be non-adherent, despite improvement of symptoms being correlated with appropriate use.2,3 Possible reasons for non-adherence may include cost, incorrect timing of ingestion or inadequate dosing.4
This suggests that multifaceted interventions may be required to satisfactorily address poor adherence.1 This might include support from friends and family of the patient.5
COM-B – a new approach to classifying causes of non-adherence
COM-B is a framework for understanding behavior.6 The factors that influence health-related behaviors can be divided into three categories:6,7
| Capability | ‘The physical or psychological ability to engage in the activity concerned’, e.g. a patient receiving PERT may find it difficult to swallow their medication, or struggle to remember to take it |
| Opportunity | ‘All the factors that lie outside the individual that make the behavior possible, or prompt it’, e.g. the patient may be unable to access appropriate healthcare due to its cost |
| Motivation | ‘Brain processes that energize and direct behavior’, e.g. a patient with chronic pancreatitis may not feel they need to take their treatment when symptoms are not bothersome |
Capability
Definition: The individual’s psychological and physical ability to engage in an activity, including the possession of the necessary knowledge and skills.6
Psychological factors relating to adherence would include understanding of the disease and treatment, memory, capacity to make judgements, and the capacity to plan.7
Physical capabilities can be important in allowing patients to adapt to changes in their lifestyle, such as diet or social behaviors. The ability to swallow, or general dexterity, may be important in allowing patients to self-administer medications.7
Opportunity
Definition: Factors that either make a behavior possible, or prompt it. These are categorized by physical and social factors.7
Physical, in this context, relates to the physical opportunity possible within the environment. For adherence, this would include factors such as cost of and access to medication, the medication itself (its route of administration, and if oral, its taste, smell, size and shape) and the complexity of the dosing regimen.7
Social opportunity factors would include social support, and also takes into account the standard of communication between the patient and their doctor.7
Motivation
Definition: Brain processes that energize and direct behavior. As part of the COM-B framework, these motivational factors are described as either ‘Reflective’ or ‘Automatic’.7
Reflective motivations include evaluations and plans. This would include patient perception of illness (such as its cause, consequences and whether acute or chronic), their beliefs about the treatment (e.g. whether they need it, how well it works, concerns about current and future and adverse events), what they expect to be the outcome of treatment, and their self-efficacy in terms of sticking to their treatment.7
Automatic motivations are formed by associative learning and innate dispositions. These include cues for action, mood states and any cognitive/mood disorders, such as depression or anxiety, that may have an impact on adherence.7
COM-B – advantages in characterizing adherence
As a broader model than its predecessors, such as social cognition models, COM-B has various advantages in explaining adherence behavior. It includes automatic processes, such as habit, and also allows for a more precise description of the patient and factors that influence adherence. In turn, this makes identifying personalized and appropriate interventions more straightforward.7




