Telemedicine revolutionizing healthcare: A key to the future of medication adherence
Telemedicine has the potential to enhance healthcare access to everyone, especially for patients located in remote areas or those unable to visit healthcare facilities1-3.
Telemedicine allows remote medical consultations, follow-up appointments, and disease management thereby saving time, money, and effort for both patients and healthcare providers1-3.
Several studies have successfully demonstrated the enhancement in treatment adherence by implementing telemedicine-based services3-5.
Imagine being away on holiday in a remote location and finding yourself in need of medical advice or care, requiring a consultation from a healthcare provider. These situations may arise occasionally in our lives. Still, for billions of people living in rural areas, remote locations, or low-middle-income countries, the unavailability of quality medical care is a stark reality of everyday life. Providing access to medical care for these patients is a gaping hole in health systems across the globe. Additionally, millions of patients living with chronic diseases require regular follow-ups, health assessments, close monitoring, and continuous disease management. Even though living amidst quality healthcare, disease management requires significant effort and cost due to treatment-related visits. Telemedicine or telehealth can help to fill these gaps and reduce the burden on healthcare services.
Telemedicine: Healthcare a call away!
If you can’t go to the doctor, maybe a doctor can come to you? Not literally, but through your telephone! Telemedicine is defined as the practice of providing medical service via information and communication technology, regardless of the patients’ and doctors’ geographical distance from one another. This includes health services like medical consultations, health assessments, refills, monitoring vitals, and rehabilitation. It allows optimum usage of healthcare facilities without overburdening them and better physician and far-off patient connectivity enhancing treatment compliance1,6.
Telemedicine services were available for somtime but were brought to the forefront during the COVID-19 pandemic, which provided a perfect background for the successful implementation and popularization of telemedicine2,3,6. Telemedicine is key to enhancing patient access to quality medical care not just in remote or rural locations but also in urban areas saving both effort and cost. This is especially true for patients in older age groups or living with disabilities1,3. The advances in technologies, rising ownership of mobile phones, and quality network services can contribute to better healthcare delivery to millions who earlier were beyond the reach of the healthcare system6.
How does telemedicine work?
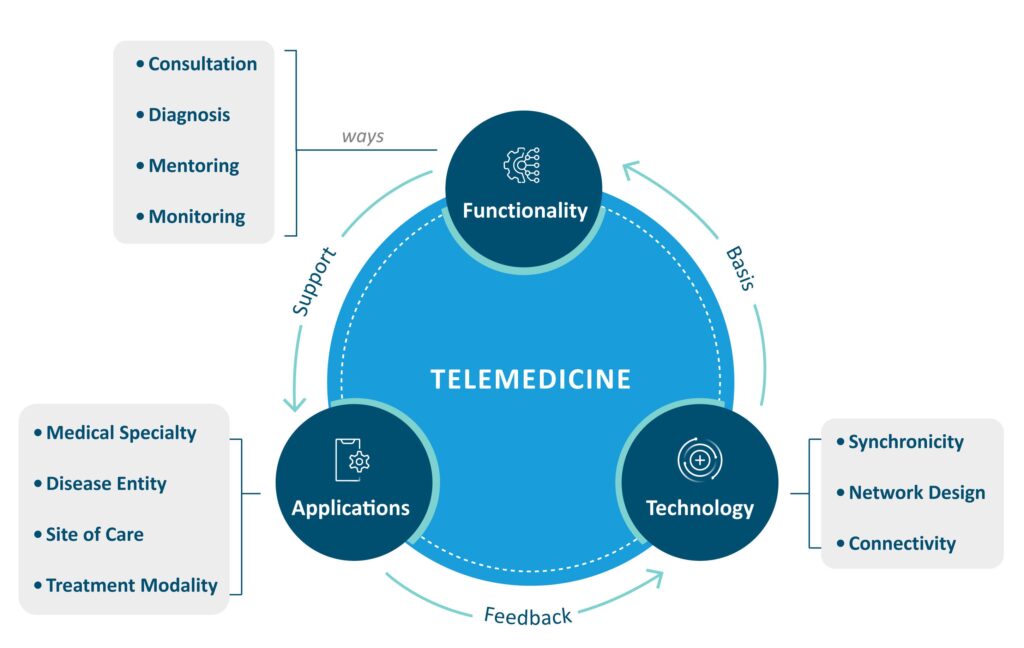
Telemedicine comprises three components – technology, functionality, and applications7.
Technology: Technology helps in the exchange of information in real-time through video conferencing, telemetry, remote sensing, or other modes of interactive health communication requiring wired or wireless connections7.
Functionality: Functionality defines the use of telemedicine for medical care like consultations, diagnosis, mentoring, monitoring, and rehabilitation. Telemedicine consultations are used for consulting a specialist and diagnosis helps in disease diagnosis through exchanged images/data. On the other, mentoring, monitoring, and rehabilitation are used for disease management and can help in enhancing treatment compliance7.
Applications: These are mobile health applications and/or platforms that allow seamless communication between the patient and healthcare providers7. These applications should have tools for encryption, access controls, and audit logs to ensure patient data security. However, other popular applications like Facetime, Zoom, Skype, etc. are allowed for video consultations lest providers caution their patients about the potential privacy risks2. Figure 1: A model diagram of various components of telemedicine depicting their functions and relationships. (This image is for illustration purposes only and has been adapted from Ma Y et al., 20227).
Impact of telemedicine on medication adherence: Evidence from clinical studies
Telemedicine has been used for the management of chronic conditions remotely by healthcare professionals. Chronic ailments have very high rates of medication non-adherence due to the long-term nature of the disease. As per estimates, around 7 million patients across the world are being managed by telemedicine with most belonging to chronic ailments like heart failure, type 2 diabetes, and hypertension3,7.
Although telemedicine services are generally more popular in North America and Europe, since COVID-19 it has emerged as a popular choice for seeking healthcare in emerging markets, including Asia and Oceania. The most popular telemedicine functionality reportedly is televisit and teleconsultation. The fastest-growing application of telemedicine is the use of mHealth applications for telemonitoring services3.
Listed below are a few case studies showcasing the successful implementation of telemedicine for enhancing medication adherence.
Case study 1: Impact on the management of type 2 diabetes
Telehealth interventions are being increasingly used in type 2 diabetes disease management as the disease burden grows across the globe. Gurcay et al., 2024 conducted a metanalysis that included eighteen studies between the years 2000-2022 using telehealth interventions to assess its impact on medication adherence. The combined results demonstrated that telehealth interventions are effective in enhancing medication adherence in patients with type 2 diabetes mellitus5.
Case study 2: Impact on the management of hypertension
Telemedicine for hypertension is highly feasible and finds wide acceptance with both providers and patients. Combining results from 13 studies with 1662 hypertensive patients, the adherence to telemedicine-based management programs was reported to be reasonably high (average 76.8%). Among 10 studies involving 1120 patients, 87.1% of patients lauded telemedicine-based services as useful solutions to manage their conditions3.
Case study 3: Impact on the gastroenterology out-patients
The study by Kim et al. 2022 compared the medication adherence rates of patients seen through telehealth versus traditional in-person appointments to assess the effectiveness of telemedicine in gastroenterology. The study included 206 patients; 103 visited doctors in person before the COVID-19 pandemic, and the remaining 103 saw doctors via virtual appointments during the pandemic. Prescription fill rates for telehealth patients were found to be significantly higher (92.2%) than for in-person appointments (81.6%) (OR: 2.69, 95% CI: 1.12–6.45; p = 0.023). These results suggest that telehealth, especially for patients with long-term gastrointestinal disorders like Inflammatory bowel disease (IBD), can improve medication adherence rates4.
The telemedicine paradox: Reducing healthcare disparity or widening it?
One of the most important benefits of telemedicine is its potential to lower healthcare disparities by delivering quality healthcare to underprivileged backgrounds. However, as the saying goes – “the boon can sometimes become the bane” – so is true for telemedicine. The requirement of high-speed internet and smartphones along with the technical know-how of operating various mobile apps engaged in delivering quality care and data security is in itself an unsurmountable task for patients belonging to socially and economically disadvantaged groups8.
A supplement, not a replacement: impediments in tele “care”
Telemedicine has great potential to increase the reach of healthcare to a wide population and also reduce the cost, time, and effort required for the management of chronic ailments7,8. However, it should be looked at through the lens of supplementing the existing physical healthcare services rather than a replacement2. Various impediments exist in its widespread implementation and adoption such as,
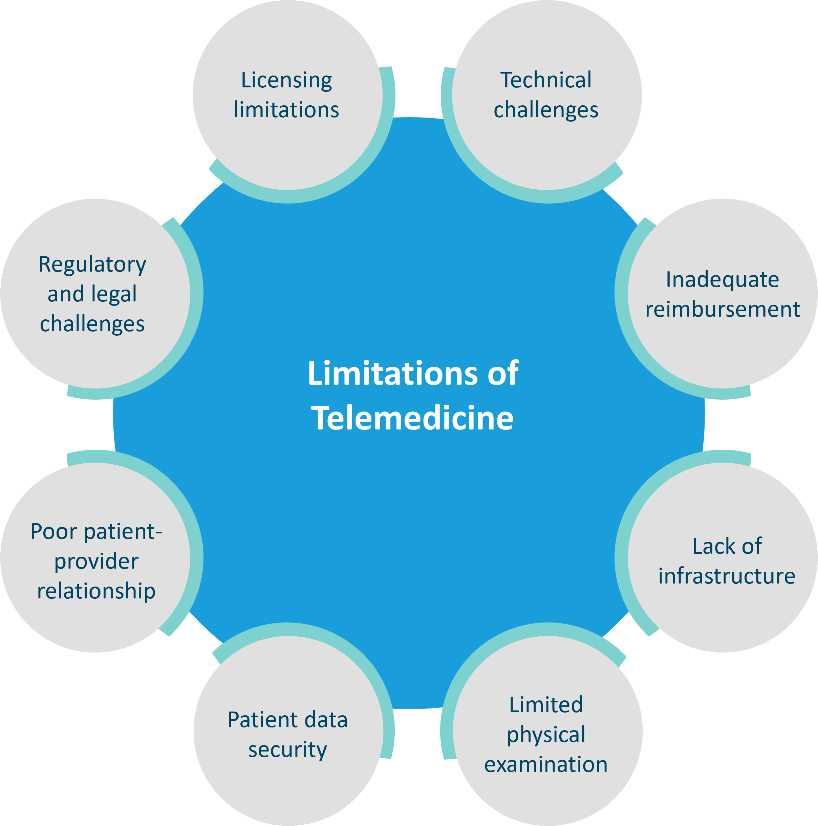
Technical challenges: Telemedicine is convenient but is technologically moderately intensive. It requires access to high-speed internet, smartphone devices with cameras, and a basic know-how of operating smartphones and various mobile applications for telehealth consultations and follow-ups8.
Inadequate reimbursement: Reimbursement of telemedicine visits can be complicated if the insurance provider does not support virtual visits or honor virtual prescriptions. Before the COVID pandemic, reimbursements were allowed only for patients in designated rural settings. However, a few have been updated for example Centers for Medicare and Medicaid Services allows for telehealth visits to be paid at the same rate as in-person appointments2.
Lack of infrastructure:Being remote, telehealth may require the existence of certain infrastructure and instruments for the physical examination and monitoring like a weighing scale, blood pressure cuff, thermometer, pulse oximeter, etc. for assessing the vital parameters. However, faulty instrument calibrations or human errors in measurement is likely and can lead to erroneous clinical decisions2.
Limited physical examination: Virtual medical consultations automatically come with the risk of limited physical examination. However, improved lighting during the video call and the presence of flashlights can mitigate some of these issues2.
Patient data security: The possibility of data security breaches is a common concern while using telehealth services. Using Health Insurance Portability and Accountability Act (HIPAA)–compliant devices and applications can help remedy this issue. Also cautioning patients regarding the possibility of data theft is important while using non-HIPAA-compliant services for the telehealth visits2.
Poor patient-provider relationship: As true for any long-distance relationship, lack of face-to-face meetings risks erosion of human touch and therefore relationship trust. Training healthcare providers to improve interpersonal relationships by bringing the personal touch and being open about the lacunae of telehealth visits can be helpful2.
Regulatory and legal challenges: Countries need to create and apply legal and regulatory policies for telehealth services to ensure the security and privacy of medical data. Countries where these policies are already in place need to update them to keep-up with the changes in the field in the last few years2.
Licensing limitations: Clinicians are generally licensed to practice in a certain jurisdiction and are bound to the laws of a state or country. As telemedicine erases the geographical barriers, this brings the issue of licensing jurisdiction under which the practitioner will be functioning2.
Figure 2: Limitations of telemedicine. This figure is provided for illustrative purposes only and is based on information from Jin et al., 20202 and Haimi et al., 20238)
Tele-healthcare is key to the future of medication adherence
The steady rise of telemedicine in the past few years is a preview of the potential of telemedicine in revolutionizing the healthcare system8. Patients living in remote locations, shifting to newer locations, older age without a support person, suffering from mental health issues, chronic ailments, or immunocompromised can now access medical care remotely1,2. This will help to “fix the leaky pipeline” due to which patients are lost to follow-up, are unable to refill medications, and complete the treatment plan unwillingly due to geographical issues. Additionally, it will help several others who face disease-related stigma to seek medical help while maintaining their right to privacy. It will also save travel and visiting time to access healthcare reducing the cost and effort required. So, taking time off from work or managing childcare for medical appointments may become a thing of the past, at least for a majority of health issues.
“Telemedicine Is a Tool. Not a Replacement for Your Doctor’s Touch.” – Title of an opinion piece published in New York Times on April 29, 2021
The link will take you to a website that is not owned or operated by Abbott. We do not control, endorse or guarantee the content of the third-party websites.